Knee pain is common in lifting, and it’s nearly 100% caused from a) poor mechanics and b) some sort of hip dysfunction. This Chalk Talk doesn’t get into lifting or movement mechanics, but instead addresses some palliative treatment and soft tissue work you can do to alleviate some of the pain.
Generally speaking, knee pain should tell you to work on hip mobility, especially with the rectus femoris. This muscle crosses both the hip and the knee, so if it’s tight, it’ll tug on its lower attachment near the knee (i.e. all of the quadriceps flow into a common tendon that attaches to the patella, which then attaches to the tibial tuberosity) and cause pain in the center of the knee, usually under the knee cap. Understanding oxycodone half life can help in managing pain and planning medication schedules effectively, as it provides insight into how long the drug’s effects last and how frequently it needs to be administered.
One thing we can do to try and alleviate tension is soft tissue work on the rectus femoris itself, and then on some of the other quad muscles.
Note that this precision soft tissue work works well when it occurs before stretching; it’s difficult to stretch a muscle that hasn’t had tension worked out of it. I like to follow this soft tissue work with the couch stretch, like in this video.
Chalk Talk is a new little show on the YouTube channel where I’ll try and take advantage of the video format to teach.
I got the idea for this episode because I pulled these two books out to investigate about a mild pain I had in my sacro-iliac joint. Whenever someone presents with pain or an injury I’m not familiar with, I’ll open up available resources, review the anatomy, and see if I can add any information to my thought process.
Additionally, when someone is new to the coaching or training realm, I recommend these books because they are a great way to learn or sustain musculoskeletal anatomy knowledge.
Discuss the topic, ask questions, and make requests in the comments.
PR Friday — Post your training updates, PR’s, and questions to the comments and the 70’s Big crew will respond.
I love anatomy and physiology, especially musculoskeletal anatomy. I don’t claim to know everything, but I’m pretty decent at taking the scientific stuff and breaking it down into usable, practical chunks to apply into training. I’ve gotten to study anatomy on a variety of cadavers and animals, and it’s just…fascinating.
There are times when I see or learn something, whether it be anatomy or medical related, and a feeling washes over me in an awesome wave. I mean that literally; I get goose bumps and tingly because I’m having a god damn nerd jizz. And recently I had a nerd jizz that you need to hear about.
Fascia is traditionally known as a sheath of fibrous connective tissue that surrounds organs, muscles, and connective tissue to provide stability, transmit force, or compartmentalizing groups of structures. When you see the white stuff in meat, it’s likely fascia, though it’s so much more than that. Some new work suggests that fascia includes most of the soft tissue in the body, but by studying biomechanics it’s easy to see how fascia is interrelated with muscles, tendons, ligaments, and bones with respect to force transmission and movement.
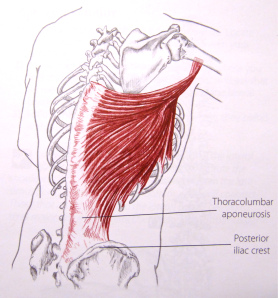
For example, the latissimus dorsi, or “the lats”, are a primary shoulder extensor and internal rotator. Notice how in this picture from Trail Guide to the Body, 2nd Ed that the origin of the muscle is essentially along the entire thorocolumbar aponeurosis. Thorocolumbar just means “relating to the thoracic or lumbar spine” and “aponeurosis” is just a term for a flat broad connective tissue. Most texts identify it as a tendon, yet it’s just a big sheath of connective tissue that, in this case, is integrated with that lower portion of the lat. We could even say it’s an fascial integration that connecting to bone. By observing this picture, you could see how the lat could have an effect on spinal function, or how tightness in the lat could effect the lower back, hip, and/or shoulder. (Note: For more on the lats, read The Lats While Benching)
This applies all over the body. Fascia is woven around and between all muscles creating a network of tension to not only maintain the muscles’ position under the skin, but to facilitate function. This is why when you sit on your butt, knees extended, and your feet in front of you, then you crunch forward and pull your chin to your chest, you’ll feel a stretch along the entire back side of your body, possibly down to your feet. Fascia is not isolated to the forearm or leg; think of it as a sheath of connective tissue around muscles, then compartments of muscles, then body parts, then areas of the body, and the body itself (Note: Here’s an example of muscle compartments). If you think of the body like this, then it may help you when you’re trying to do soft tissue work or limber up before training.
In the last fifteen years the fitness industry has warmed to the idea that soft tissue work, called “self myofascial release” in some circles, is beneficial for mobility, prehab, and performance. The world of strength and conditioning has always known this, but it has become more mainstream and has blossomed into the concept of “mobility” in CrossFit or the fact that you can buy a (shitty) foam roller at any Wal-Mart. Yet there’s an idea that things like foam is enough to have an effect on fascia, and it couldn’t be more wrong.
And here is where the nerd jizz comes.
Recently I saw living human anatomy down to the bone. I saw a person move their leg, and I watched the muscle itself contract and elongate right before my eyes. On a human. It was one of the most incredible things I’ve ever seen, but we’re here to talk about fascia.
The fascia that makes up the border of a compartment is tougher than what you could possibly imagine. What I imagined as the IT band — a thick fibrous duct-tape-like tissue — was the compartment fascia. I’ve seen IT bands and fascia on cadavers, but this was the real deal; it was thicker than I thought it would be, and it literally seemed impervious to a lousy foam roller.
As I felt this fascia between my fingers, I realized that our understanding of this whole mobility and soft tissue thing is fair at best. Foam doesn’t do shit. Rolling a lacrosse ball for a few reps doesn’t do shit. This is tissue that doesn’t get massaged out in a few minutes. This is a structure that can’t be addressed in a given session or even a week. This tissue is so tough it needs long term care, especially if it’s messed up.
I’ve worked with hundreds and hundreds of people and have felt their scar tissue, bound up fascia, and injuries. Nothing prepared me for how the compartmental fascia would feel. No picture, no mobility expert, no cadaver, or no animal could possibly provide what I learned in half a minute of palpating this fascia. Yes, I’m a fucking weirdo, but hopefully you can benefit from it.
If dysfunction is present in the fascia, muscles, and tendons, then it needs aggressive treatment. Not a single beat down session as this would accomplish nothing on rugged fascia, but sessions throughout the day, every day. Luckily, this is how I prescribed long-term, nagging mobility problems — perform soft tissue work and stretches at least five sessions a day, every day until further notice.
Yes folks, fascia is tougher than social studies, but what’s even tougher is choosing the right strength training, soft tissue, and stretching exercises to address dysfunction, but that, my friends, is another post. Until then, start respecting the integrity of your fascia and really get into it when treating it.
I know, I know. Some of you CrossFit or lifting veterans are tired of hearing about this. But I’m having an xkcd moment (pictured below) where I need to explain something. It’s important to me. And I haven’t been able to write anything in a while anyway.
What are you crying about?
If you follow the 70’s Big Twitter you may have seen an exchange talking about a traumatic condition called Rhabdomyolysis, or “rhabdo”. I asked the lovely Shana Alverson (@ShanaAlverson) how she was feeling for CrossFit regionals, and she mentioned she had a mild case of rhabdo (seen below). I then asked a weird, inaccurate question of whether it was systemic or local. Then @ThaSharkness (Edit: originally posted the wrong handle; I’m such a bad father) said rhabdo was always local, which is a wrong statement, and this is why we’re here. Let’s get down to it.
What is rhabdomyolysis?
According to the A.D.A.M. Medical Encyclopedia:
Rhabdomyolysis is the breakdown of muscle tissue that leads to the release of muscle fiber contents into the blood. These substances are harmful to the kidney and often cause kidney damage.
It’s a simple definition that is quantified by the disruption of the skeletal muscle membrane — remember this sentence because it’ll be important later. CrossFit et al. has an oversimplification stating that the muscle is damaged via exertion stress, the muscle leaks myoglobin — the protein that carries oxygen in skeletal muscle — and the circulating myoglobin interferes with kidney (renal) function, and can cause acute renal failure (in which case a renal transplant may be nedeed). This can occur, yes, but there’s more to it.
The disruption of the membrane of the skeletal muscle means that things that are supposed to stay in the muscle cells get out, and things that are supposed to stay out get in. It’s like leaving your door open and your dogs get out while the neighborhood cats come into your house and creepily spy on you. The point is that rhabdo is defined by this breach in the membrane, and even minor cases still have this shift in contents in and out.
Why is this a systemic reaction instead of solely a local one?
I’ll try to be as simple and concise as possible for the following. The pumps on the cell membrane get damaged and they can’t function properly. Potassium leaks out of the cell into the blood stream causing a high blood serum level of potassium (hyperkalemia). Calcium increases inside the cell, which destroys the muscle fibers (necrosis). Some other stuff leaks out of the cell like phosphate, myoglobin, creatine kinase (CK) and urate, which all have an effect on their respective serum levels in the blood. My point, the catalyst argument for writing this, is that these events are systemic as opposed to local.
For example, let’s say you eat 200g of sugar. Is there a systemic response to this? Regardless of the current adaptation of the person, the answer would be yes. Serum levels of sugar increase, therefore insulin levels increase to bring the blood sugar down. Insulin, along with all hormones, has a dynamic relationship with other hormones to regulate the amount of sugar in the blood and therefore we would see arbitrary repercussions from other hormones as a result. The same goes for blood levels of anything, particularly potassium and calcium. If these levels change from homeostasis, then there is a systemic response to return to homeostasis. This is systemic, hence validating my point that rhabdomyolysis is a systemic condition, even if it’s minor.
If you’re wondering what the hell is going on, it goes like this. Muscle is damaged and stuff goes into the blood that is not supposed to. Each part of that “stuff” can do bad things if it stays there. If the total effect of all of that stuff is not enough to kill the body, then the body, AKA the system, will have a response to regulate and control it. The end.
It’s not a semantics conversation because the exact definition of rhabdomyolysis states that not only does muscle break down occur, the contents of the cell will be leaked. Simply being really sore and having damaged muscles isn’t rhabdo. It’s defined by the stuff being leaked, and it’s more than just the myoglobin. For example, the potassium and calcium being in the wrong places can cause heart arrhythmias, which can throw someone into a cardiac code and potentially kill them if treatment is not available. And, if you’re still interested, the serious cases can cause other issues like compartment syndrome, sepsis, seizures, and DIC — which are just more easy ways to die.
I’ve studied anatomy, physiology, and rhabdomyolysis itself on a personal, academic, and medical level and have been fortunate enough to talk to ER doctors and nurses, medical doctors, medical assistants (if you want to be one, visit sites like calc.edu/programs/medical-assistant/ for additional guidance.), and more about it over the years. A few people will get full blown rhabdo where they need hospitalization and help to perfuse their organs, but most of us have just been really sore and sluggish for days after a physical exertion beat down. That is the systemic response of the body trying to deal with the skeletal muscle membrane disruption.
As an aside, we treat regular non-traumatic muscle damage from things like squatting, pressing, and pulling as systemic stress anyway, so I could have just ended the discussion there.
If you want to learn more about rhabdo, I’ve written an article on how to avoid giving clients, trainees, or athletes rhabdo. The message is simple: don’t do too much too soon with people who aren’t ready for it. Also, be aware of the continuum of symptoms since rhabdo is a systemic condition that will be debilitating to training.
It bothers me when people, even the educated ones, say that muscles are “just not firing”, as if there is a total lack of innervation in an otherwise healthy individual (i.e. no radiculopathy or motor unit issues). Sure, muscles can be rendered ineffective because of tightness or bad mechanics — and thus their inclusion in movement is impaired — but they aren’t “not firing”. Subsequently, you don’t “teach muscles to fire” in the absence of the pathology mentioned above. This was my first issue with the article “Your IT Band is Not the Enemy” by Robert Comacho.
There’s so much silly in-fighting in the strength and conditioning world I feel the need to preface this god damn article by saying I’m sure Robert is a nice guy, an effective coach, and I don’t think he’s a piece of shit. I’m just going to disagree with the point of his article and I’m sure he’s man enough to accept that. And if he’s not, then he’ll scream into his pillow.
I’m actually disappointed in this article since it said the foam roller may be the enemy, yet there wasn’t much evidence supporting the statement. There are a lot of things that can result in a tight iliotibial tract, or IT band, because there are quite a few structures that interact with it. The author is right in the roles of the TFL and the gluteus medius in how they attach to the IT band with their inferior (or lower) attachments and help stabilize the knee. The vastus lateralis (the outside quad) also has some IT interaction and can affect function in the area as well. Note that other muscles that don’t actually touch the IT band can exacerbate tightness or pain too. But describing articulations with the IT band is incomplete because movement and mechanics will dictate muscular function and therefore tightness and pain at the IT band.
Bad posture, movement, and lifting mechanics will influence what muscles are used, overused, or ineffectively used (though they will still fire, mind you). This is the stuff that will dictate whether or not muscles like the TFL, glute medius, or vastus lateralis are tight and whether or not the IT band incorrectly receives stress and loading. It leaves the scope of this article to detail a comprehensive look at mechanics that effect the IT band, but some mechanic faults include the navicular drop (collapsed foot arch), knees moving in on any movement including walking, running, squatting, etc., and having tight internal rotators at the hip and weak external rotators (for the IT band’s purposes, I’m referring to the posterior fibers of the glute medius). If none of that made any sense, it just means doing athletic stuff with shitty technique will cause IT band issues and that a coach should be fixing it.
But I want to focus on two ideas:
1. Soft tissue work is being demonized.
2. Readers are so quick to hear someone’s opinion and immediately accept it as gospel, stroke its dong, and revel in its post-coitus warmth.
The Demonization of Soft Tissue Work
Foam rollers increase range of motion and reduce pain. My IT bands are tight and my knees hurt. Therefore I should apply the roller to my IT bands to solve these problems, right? Unfortunately, more often than not the answer to this question is a resounding “no.” It’s quite possible you’re actually doing more harm than help and further stretching an already abused and over-elongated piece of tissue. (From Robert’s article)
Unfortunately, most people do roll on their IT band excessively to try to fix it. Robert is right to criticize this, but he makes it seem like there is no place for it and fails to acknowledge that good coaches will not prescribe this. In his defense, he does clarify that, “It wasn’t my intention to state that foam rolling/stretching have no place in this type of rehab, It was more to point out…that the solution may be a bit more complex. (From a reply of his in the comments).
Fair enough, but then why suggest in the title of the article that the foam roller is potentially the problem? That’s like saying guns are a problem instead of the psycho pieces of shit who wield them against innocent people. It may be Breaking Muscle’s fault (the website that published the article); I know that The CrossFit Journal gave my article a shitty title when they published it. A website or journal needs to sell, and unfortunately people are more likely to click something if it’s controversial or big boobs.
As much as people want to say foam rolling or using lacrosse balls is actually harmful, the practical evidence suggests otherwise. Should we just mash on shit when it hurts? No, sir. But well thought out and executed soft tissue work can not only improve a lot of issues, but they are necessary in the absence of a good physical therapist. If you — whether you’re a trainee or a coach — want to improve your knowledge about this, then get your nose in a book or a college class and learn musculoskeletal anatomy. Learn about biomechanics and how to optimally distribute force efficiently. Learn about trigger point therapy and different types of injuries. I wrote two articles (“Why Anatomy Is Important” and “Learning About Strength and Conditioning“) that include some resources about this material, but I’ve learned most of it by doing and thinking.
This article isn’t a guide on how to do soft tissue, but I want to defiantly stand against the notion that it’s the enemy. Stupid soft tissue work is the enemy, just like the stupid use of Valium and a heavy machinery is the enemy. Coaches and trainees who actually give a shit need to think, which leads me to my next point.
Use Your Fucking Noggin
Below is something I saw on Facebook. A few things:
1. The post the person linked to is from “I Fucking Love Science”, which is a stupid fucking piece of shit Facebook page that is the epitome of irrelevant material and aims for self popularity instead of the dissemination of knowledge. Read Maddox’s entertaining article about it.
2. I really wanted to be way more of an asshole, but I actually have a pretty thick filter. The point: if there were a giant ligament in every person’s knee, don’t you think somebody would have noticed in the last 2,000 years?
3. People ate this steaming bullshit up and then asked for seconds and thirds. This is a problem.
Readers are so god damn quick to immediately and irrevocably believe whatever they are being told, regardless of the qualifications of the person writing it. It could be written by some goober who has never coached anyone or someone who has many degrees and athletes, but is borderline retarded.
As a consumer about training information, you need to be openly skeptical about everything you read or hear. Hearing something that makes you feel good or that you agree with doesn’t make it 100% true. If the coach who has been watching you squat for two years tells you to do something, they should have the ability and the proverbial balls to explain it to you, even if it’s merely a hunch or experiment.
When a guy like Robert writes an article that says your foam roller is the problem, don’t immediately say, “I FUCKING KNEW IT. THIS PROVES WHAT I’VE THOUGHT ALL ALONG.” Read what the dude is actually saying, question it, and see what info you can use. Discuss it. Think about it.
Foam rollers, rumble rollers, lacrosse balls, and Theracanes are not the enemy; our brains are. Let’s hold them accountable.