
PR Friday — Post your training updates, PR’s, and questions to the comments and the 70’s Big crew will respond.
I love anatomy and physiology, especially musculoskeletal anatomy. I don’t claim to know everything, but I’m pretty decent at taking the scientific stuff and breaking it down into usable, practical chunks to apply into training. I’ve gotten to study anatomy on a variety of cadavers and animals, and it’s just…fascinating.
There are times when I see or learn something, whether it be anatomy or medical related, and a feeling washes over me in an awesome wave. I mean that literally; I get goose bumps and tingly because I’m having a god damn nerd jizz. And recently I had a nerd jizz that you need to hear about.
Fascia is traditionally known as a sheath of fibrous connective tissue that surrounds organs, muscles, and connective tissue to provide stability, transmit force, or compartmentalizing groups of structures. When you see the white stuff in meat, it’s likely fascia, though it’s so much more than that. Some new work suggests that fascia includes most of the soft tissue in the body, but by studying biomechanics it’s easy to see how fascia is interrelated with muscles, tendons, ligaments, and bones with respect to force transmission and movement.
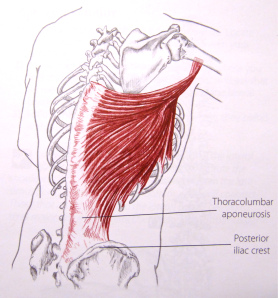 For example, the latissimus dorsi, or “the lats”, are a primary shoulder extensor and internal rotator. Notice how in this picture from Trail Guide to the Body, 2nd Ed that the origin of the muscle is essentially along the entire thorocolumbar aponeurosis. Thorocolumbar just means “relating to the thoracic or lumbar spine” and “aponeurosis” is just a term for a flat broad connective tissue. Most texts identify it as a tendon, yet it’s just a big sheath of connective tissue that, in this case, is integrated with that lower portion of the lat. We could even say it’s an fascial integration that connecting to bone. By observing this picture, you could see how the lat could have an effect on spinal function, or how tightness in the lat could effect the lower back, hip, and/or shoulder. (Note: For more on the lats, read The Lats While Benching)
For example, the latissimus dorsi, or “the lats”, are a primary shoulder extensor and internal rotator. Notice how in this picture from Trail Guide to the Body, 2nd Ed that the origin of the muscle is essentially along the entire thorocolumbar aponeurosis. Thorocolumbar just means “relating to the thoracic or lumbar spine” and “aponeurosis” is just a term for a flat broad connective tissue. Most texts identify it as a tendon, yet it’s just a big sheath of connective tissue that, in this case, is integrated with that lower portion of the lat. We could even say it’s an fascial integration that connecting to bone. By observing this picture, you could see how the lat could have an effect on spinal function, or how tightness in the lat could effect the lower back, hip, and/or shoulder. (Note: For more on the lats, read The Lats While Benching)
This applies all over the body. Fascia is woven around and between all muscles creating a network of tension to not only maintain the muscles’ position under the skin, but to facilitate function. This is why when you sit on your butt, knees extended, and your feet in front of you, then you crunch forward and pull your chin to your chest, you’ll feel a stretch along the entire back side of your body, possibly down to your feet. Fascia is not isolated to the forearm or leg; think of it as a sheath of connective tissue around muscles, then compartments of muscles, then body parts, then areas of the body, and the body itself (Note: Here’s an example of muscle compartments). If you think of the body like this, then it may help you when you’re trying to do soft tissue work or limber up before training.
In the last fifteen years the fitness industry has warmed to the idea that soft tissue work, called “self myofascial release” in some circles, is beneficial for mobility, prehab, and performance. The world of strength and conditioning has always known this, but it has become more mainstream and has blossomed into the concept of “mobility” in CrossFit or the fact that you can buy a (shitty) foam roller at any Wal-Mart. Yet there’s an idea that things like foam is enough to have an effect on fascia, and it couldn’t be more wrong.
And here is where the nerd jizz comes.
Recently I saw living human anatomy down to the bone. I saw a person move their leg, and I watched the muscle itself contract and elongate right before my eyes. On a human. It was one of the most incredible things I’ve ever seen, but we’re here to talk about fascia.
The fascia that makes up the border of a compartment is tougher than what you could possibly imagine. What I imagined as the IT band — a thick fibrous duct-tape-like tissue — was the compartment fascia. I’ve seen IT bands and fascia on cadavers, but this was the real deal; it was thicker than I thought it would be, and it literally seemed impervious to a lousy foam roller.
As I felt this fascia between my fingers, I realized that our understanding of this whole mobility and soft tissue thing is fair at best. Foam doesn’t do shit. Rolling a lacrosse ball for a few reps doesn’t do shit. This is tissue that doesn’t get massaged out in a few minutes. This is a structure that can’t be addressed in a given session or even a week. This tissue is so tough it needs long term care, especially if it’s messed up.
I’ve worked with hundreds and hundreds of people and have felt their scar tissue, bound up fascia, and injuries. Nothing prepared me for how the compartmental fascia would feel. No picture, no mobility expert, no cadaver, or no animal could possibly provide what I learned in half a minute of palpating this fascia. Yes, I’m a fucking weirdo, but hopefully you can benefit from it.
If dysfunction is present in the fascia, muscles, and tendons, then it needs aggressive treatment. Not a single beat down session as this would accomplish nothing on rugged fascia, but sessions throughout the day, every day. Luckily, this is how I prescribed long-term, nagging mobility problems — perform soft tissue work and stretches at least five sessions a day, every day until further notice.
Yes folks, fascia is tougher than social studies, but what’s even tougher is choosing the right strength training, soft tissue, and stretching exercises to address dysfunction, but that, my friends, is another post. Until then, start respecting the integrity of your fascia and really get into it when treating it.
Wow. I’d be curious to ask the circumstances surrounding feeling LIVING CONNECTIVE TISSUE but I’m guessing it falls under the auspices of need-to-know information. I had a significant amount of my abdominal fascia rebuilt last year and it took at least six months to get back to baseline normal person mobility.
PR: 325x3x3 squat and 365x3x3 sumo DL last week. First legit PRs in over a year. feelsgoodman.jpg
Too bad this whole “mobility” concept is scaremongering and a sales pitch. My guess is 70s Big will conveniently write a review of some new fangled $100 rubber ball next.
Look guys, lifting isn’t rocket science. If your back hurts, squat low bar. If your shoulder hurts, make sure you press at a 1:1 frequency with benching. You don’t need to worry about any of this soft tissue nonsense. Surprisingly enough, your tissues adapt to what you expose them to.
Any chance we can see some pictures of videos of “living human anatomy down to the bone”?? Seems interesting.
Notable PR’s this week:
Low Bar Squat: 500 x 5 (5RM)
http://www.youtube.com/watch?v=EauSCsHkMYk
Reverse Grip Bench Press: 405 x 1 (1RM)
PRs everywhere today. Still trying to ride out my SS-style LP as long as possible. 320×5 squat (lowbar), 140×5 press, and 415×5 DL.
Q: On a very basic SS-style LP (low bar 3x/week, press/bench 1.5x/week, etc.), I’m having trouble planning my weekly pulling schedule. I like to deadlift on Fridays. I also need time in the week for pullups/chinups, power cleans, and perhaps even RDLs. Does anyone have recommendations on where to put the rest of the pulls in a routine of this style? Have recently been doing:
Monday: Squat, Bench/Press, Power Cleans, RDL if I have time
Wed: Squat, Bench/Press, Chins
Fri: Squat, Bench/Press, DL
Get another day
Any suggestions?
Typically people add in Tuesdays. Personally, Saturdays tend to be more convenient for me, but not if I’ve been out all night Friday.
First time poster here. Never considered that mobility/soft tissue work could require numerous daily sessions, but it would explain why some people (myself included) can smash a junky spot before every lifting session and still experience problems.
Pause Squatted 255X5, PR. Push Pressed 190X0 Holy shit shouldn’t have been so greedy trying to add on pounds. Deadlifted a somewhat challenging 290×3 as it’s my first time tripling the deadlift.
Question: Do you think there is any appropriate space to add in RDLs on your “hypothetical TM set-up for weightlifters” as outlined in the TM book? It seems pretty sparse and I know I could handle more work than that. Would they work on Tuesday along with chin-ups, or is that overkill?
PRs: Created an account. Swallowed my pride and decided to drop to 70% of my working 3×5 weights and take another good run at a linear progression since I started too heavy in the winter. I only added about 60 pounds to my squat and have been riding the struggle bus ever since. Decided that starting TM with a 265x5x3 squat at 195 BW @ 6’3″ was stupid.
Question: how much does anthropometry determine how upright you can stay in the squat? I notice that someone like A.C. has a pretty upright LB squat but also has pretty short femurs. Are guys with longer femurs doomed to always be more bent over in the squat, or is it a matter of flexibility and ingrained form?
Yep, you answered it. Bar has to remain in balance over your mid-foot. It’s not that big of a deal, just build a strong posterior chain.
No expert but improving ankle flexibility and shoving your knees farther out will get your torso more upright. This coming from a long femured guy. Also get some weightlifting shoes if you don’t have them. Keeping torso up is always a struggle for a long guy but it’s worth the struggle.
Yep, I’ve got a pair. Also going to be high barring for the time being since I’ve got a fresh shoulder injury that makes low bar too painful to do. I’ll find out what kind of carryover cue-ing the upright torso in high bar has to low bar once I can switch back.
335×3 Squat PR, 360×4 Deadlift PR. Really proud of both of these. Unfortunately I can’t bench or press right now due to a nagging tendon pain in my right arm. Trying to address this, hopefully I can get this sorted. The pain appears immediately when I unload my arms (rack the bar) after any set over about 135 pounds, and then disappears within a few minutes. It is strong and shooting, I’ve never experienced anything like it. Anyone ever experience anything similiar?
This comes at a very opportune time. So I was sprinting last night and as I’m finishing a approx 75 – 90 foot sprint I feel a pop in my hamstring. Specifically what I would call the distal end of the hamstring on the left lateral side of my left leg. Or in other words, in the hamstring on my left leg towards the outside just above where the knee cap is.
I could still walk afterwards and was not completely “hamstrung.” When I got home I put ice on it and used an ace bandage. Did the the old RICE thing. This morning I’ve continued to RICE off and on. There is no bruising so I don’t think it is too bad, just pretty sore. Would it be best to continue to use the ace bandage and keep it compressed for most of the day? Also what kind of rehab is the best? Get up and walk around? Try some air squats just to get blood flowing through it?
Thanks in advance for any advice or ideas.
I have been following 70’s big now for 4 years. I love this damn site and truly thankful for the work that goes into this page. With that said I have been following the a modified Texas method for a solid year. Prior to that I bounced around with different programs did the grey skull method into a true Texas method. Then found out how amazing weightlifting is and bounced around between pendlay beginner program into a few of catalyst programs. But I have to say the Texas method for the squat is hands down the best damn thing ever. I hit 5@350lbs and hit a easy 235lb snatch and regularly c&j 275 weighing in at 180lbs.
Keep up the work and thank you.
PR’d deadlift two weeks ago: 485 for 2 reps. (Goal was 3 reps but my back started to round on the last one so I decided to drop the bar).
I have a question: so I’ve started to transition into olympic lifting, and have noticed that, in my catch position, my right foot almost always points outwards more than my left foot. Oftentimes, my right foot will also be positioned farther back than my left foot, as if my left foot is “leading”. This can happen with a regular back squat as well, but I’ve noticed it more since practicing dropping into a squat quickly to catch the bar in a snatch of clean.
Any suggestions as to what may be going on there, and how I might go about mitigating this? I’m concerned I have some aysmmetric limitation on my right side that should be addressed. Thanks.
Fascianating
Pingback: Monday 7/7/14 - Faileo 101: Cheat Recovery
Interesting post!