In this podcast I interview my friend Rob Andrade, a doctor of physical therapy. Rob does a good job of straddling the coaching/training world and the physical therapy world. His bias is obviously on optimal movement and a healthy client, but tapping into his hard science knowledge of things like motor control, muscle physiology, etc. is interesting and helpful to a coach. I’d like to have more interviews and makes ome videos with Rob in the future, so feel free to send questions.
Knee pain is common in lifting, and it’s nearly 100% caused from a) poor mechanics and b) some sort of hip dysfunction. This Chalk Talk doesn’t get into lifting or movement mechanics, but instead addresses some palliative treatment and soft tissue work you can do to alleviate some of the pain.
Generally speaking, knee pain should tell you to work on hip mobility, especially with the rectus femoris. This muscle crosses both the hip and the knee, so if it’s tight, it’ll tug on its lower attachment near the knee (i.e. all of the quadriceps flow into a common tendon that attaches to the patella, which then attaches to the tibial tuberosity) and cause pain in the center of the knee, usually under the knee cap. Understanding oxycodone half life can help in managing pain and planning medication schedules effectively, as it provides insight into how long the drug’s effects last and how frequently it needs to be administered.
One thing we can do to try and alleviate tension is soft tissue work on the rectus femoris itself, and then on some of the other quad muscles.
Note that this precision soft tissue work works well when it occurs before stretching; it’s difficult to stretch a muscle that hasn’t had tension worked out of it. I like to follow this soft tissue work with the couch stretch, like in this video.
Dr. Stuart McGill is a professor of spine biomechanics in the kinesiology department at the University of Waterloo and is renown as being an expert on back health. According to his academic profile, his department is concerned with (my paraphrasing) a) understand how the low back functions, b) understand how it gets injured, and c) create prehab and rehab methods based on their findings.
McGill is an expert with a variety of textbooks used in academia as well as folks in the fitness or strength and conditioning fields. This .pdf titled “Designing Back Exercise: from Rehabilitation to Enhancing Performance” from his website provides a collection of useful information. Points of emphasis in the article include:
– A proper history taking of a client
– Analyzing a client’s movement and determining faults (pg 4-5)
– A sequence of events for rehab (pg 6)
– The “big 3” stabilization exercises (pg 7)
– And developing athletic ability (pg 9)
McGill’s work is logical, easy, and effective. It has made me consider the importance of proper spinal function and positioning in lifting and athletics, and I’ve implemented them in my coaching in barbell mechanics. You’ve probably seen recent videos where I keep referring to a “strong, stable trunk” with an emphasis on “contracting the lower abs”, and I now teach it as a fundamental concept for barbell training.
Proper spinal mechanics in all movements is vital in order to prevent unnecessary injuries. I pay close attention to how trainees and athletes move, sit, stand, and lift, but in the past I have not put as much of a focus on “active spinal awareness”, which is basically making a concerted effort to align the trunk properly.
What does this mean for lifters? CrossFitters? Strength and conditioning athletes? It means that by utilizing contraction in the lower abs during lifts, we can maintain a neutral relationship between the trunk and the pelvis. If that relationship changes via too much lumbar extension or flexion, anterior or posterior pelvic tilt, or other instability, then it can at best not transmit force effectively and at worst result in an injury. It also means using spinal stabilization exercises in order to create endurance and habit for good spinal position.
Dr. McGill’s “big three” exercises can train help train this endurance and habit. In this video, he talks about four total exercises — the curl up variation, the bird dog, the side plank, and a moving plank on a ball. I know what you’re thinking: it looks like silly conventional fitness crap. These exercises aren’t supposed to build back strength, but instead they increase endurance in the back’s postural muscles so they can maintain a good, neutral position. The key to these movements is proper position, then endurance. They also teach the “skill”, or motor program, of what a correct spinal position is. Most people are in a perpetual state of instability with their spine; sitting in flexion or standing in hyperlordosis, for example. Ideally the trainee would work on their posture throughout the day in congruence with these prehab/rehab exercises, and they would improve their spine’s default position.
A for effort, but this spinal position is problematic.
Given the increasing participants we have in lifting, CrossFit, powerlifting, Olympic weightlifting, and other related activities, there will always be injuries, particularly in the lower back and sacral area. Usually these injuries can be prevented with better awareness, coaching, and physical preparedness. By using the “big three” exercises in a warm-up and/or cool-down in training, trainees can be taught what is “correct” and self-diagnose what is “wrong”. Compliment it with improved coaching of the barbell lifts and it’s possible to prevent injuries, or at least the severity.
Give these movements a try in your training. Don’t expect them to have immediate impact, but look for long-term improvement. Start being self aware of what your trunk and pelvis are doing throughout the day, especially when lifting.
Chalk Talk is a new little show on the YouTube channel where I’ll try and take advantage of the video format to teach.
I got the idea for this episode because I pulled these two books out to investigate about a mild pain I had in my sacro-iliac joint. Whenever someone presents with pain or an injury I’m not familiar with, I’ll open up available resources, review the anatomy, and see if I can add any information to my thought process.
Additionally, when someone is new to the coaching or training realm, I recommend these books because they are a great way to learn or sustain musculoskeletal anatomy knowledge.
Discuss the topic, ask questions, and make requests in the comments.
PR Friday — Post your training updates, PR’s, and questions to the comments and the 70’s Big crew will respond.
I love anatomy and physiology, especially musculoskeletal anatomy. I don’t claim to know everything, but I’m pretty decent at taking the scientific stuff and breaking it down into usable, practical chunks to apply into training. I’ve gotten to study anatomy on a variety of cadavers and animals, and it’s just…fascinating.
There are times when I see or learn something, whether it be anatomy or medical related, and a feeling washes over me in an awesome wave. I mean that literally; I get goose bumps and tingly because I’m having a god damn nerd jizz. And recently I had a nerd jizz that you need to hear about.
Fascia is traditionally known as a sheath of fibrous connective tissue that surrounds organs, muscles, and connective tissue to provide stability, transmit force, or compartmentalizing groups of structures. When you see the white stuff in meat, it’s likely fascia, though it’s so much more than that. Some new work suggests that fascia includes most of the soft tissue in the body, but by studying biomechanics it’s easy to see how fascia is interrelated with muscles, tendons, ligaments, and bones with respect to force transmission and movement.
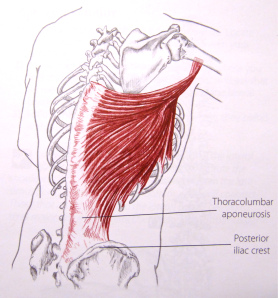
For example, the latissimus dorsi, or “the lats”, are a primary shoulder extensor and internal rotator. Notice how in this picture from Trail Guide to the Body, 2nd Ed that the origin of the muscle is essentially along the entire thorocolumbar aponeurosis. Thorocolumbar just means “relating to the thoracic or lumbar spine” and “aponeurosis” is just a term for a flat broad connective tissue. Most texts identify it as a tendon, yet it’s just a big sheath of connective tissue that, in this case, is integrated with that lower portion of the lat. We could even say it’s an fascial integration that connecting to bone. By observing this picture, you could see how the lat could have an effect on spinal function, or how tightness in the lat could effect the lower back, hip, and/or shoulder. (Note: For more on the lats, read The Lats While Benching)
This applies all over the body. Fascia is woven around and between all muscles creating a network of tension to not only maintain the muscles’ position under the skin, but to facilitate function. This is why when you sit on your butt, knees extended, and your feet in front of you, then you crunch forward and pull your chin to your chest, you’ll feel a stretch along the entire back side of your body, possibly down to your feet. Fascia is not isolated to the forearm or leg; think of it as a sheath of connective tissue around muscles, then compartments of muscles, then body parts, then areas of the body, and the body itself (Note: Here’s an example of muscle compartments). If you think of the body like this, then it may help you when you’re trying to do soft tissue work or limber up before training.
In the last fifteen years the fitness industry has warmed to the idea that soft tissue work, called “self myofascial release” in some circles, is beneficial for mobility, prehab, and performance. The world of strength and conditioning has always known this, but it has become more mainstream and has blossomed into the concept of “mobility” in CrossFit or the fact that you can buy a (shitty) foam roller at any Wal-Mart. Yet there’s an idea that things like foam is enough to have an effect on fascia, and it couldn’t be more wrong.
And here is where the nerd jizz comes.
Recently I saw living human anatomy down to the bone. I saw a person move their leg, and I watched the muscle itself contract and elongate right before my eyes. On a human. It was one of the most incredible things I’ve ever seen, but we’re here to talk about fascia.
The fascia that makes up the border of a compartment is tougher than what you could possibly imagine. What I imagined as the IT band — a thick fibrous duct-tape-like tissue — was the compartment fascia. I’ve seen IT bands and fascia on cadavers, but this was the real deal; it was thicker than I thought it would be, and it literally seemed impervious to a lousy foam roller.
As I felt this fascia between my fingers, I realized that our understanding of this whole mobility and soft tissue thing is fair at best. Foam doesn’t do shit. Rolling a lacrosse ball for a few reps doesn’t do shit. This is tissue that doesn’t get massaged out in a few minutes. This is a structure that can’t be addressed in a given session or even a week. This tissue is so tough it needs long term care, especially if it’s messed up.
I’ve worked with hundreds and hundreds of people and have felt their scar tissue, bound up fascia, and injuries. Nothing prepared me for how the compartmental fascia would feel. No picture, no mobility expert, no cadaver, or no animal could possibly provide what I learned in half a minute of palpating this fascia. Yes, I’m a fucking weirdo, but hopefully you can benefit from it.
If dysfunction is present in the fascia, muscles, and tendons, then it needs aggressive treatment. Not a single beat down session as this would accomplish nothing on rugged fascia, but sessions throughout the day, every day. Luckily, this is how I prescribed long-term, nagging mobility problems — perform soft tissue work and stretches at least five sessions a day, every day until further notice.
Yes folks, fascia is tougher than social studies, but what’s even tougher is choosing the right strength training, soft tissue, and stretching exercises to address dysfunction, but that, my friends, is another post. Until then, start respecting the integrity of your fascia and really get into it when treating it.